
For the past 12-years Down’s syndrome screening quality assurance support service (DQASS) has audited our paired crown rump length (CRL) and nuchal translucency (NT) images and measurement bias/ spread in order the safeguard the performance of the combined screening programme for trisomy 21, 18 and 13.
Each department has a Screening Support Sonographer (SSS) and a deputy whose role is to “oversee the implementation, delivery and monitoring of the ultrasound aspects of the [combined screening] service” (NHS FASP, 2014).
Every 6 months the SSS disseminates the DQASS graphs (feedback plots) for each individual sonographer, describing the bias and spread of their combined screening test measurements (CRL and NT) (NHS FASP, 2022). Green, amber and red flags are given to sonographers based on this information. An ideal feedback plot (green flag) should have 50% of measurements within the grey band around the 50th centile, 25% of measurements would be above the grey and a further 25% would be below the grey band.
Green flag
Figure 1 demonstrates a ‘green flag’ feedback plot with most measurements being within the ideal range. Sonographers should ideally aim to achieve a green flag rating, which equates to less than 0.1mm bias in measurements.
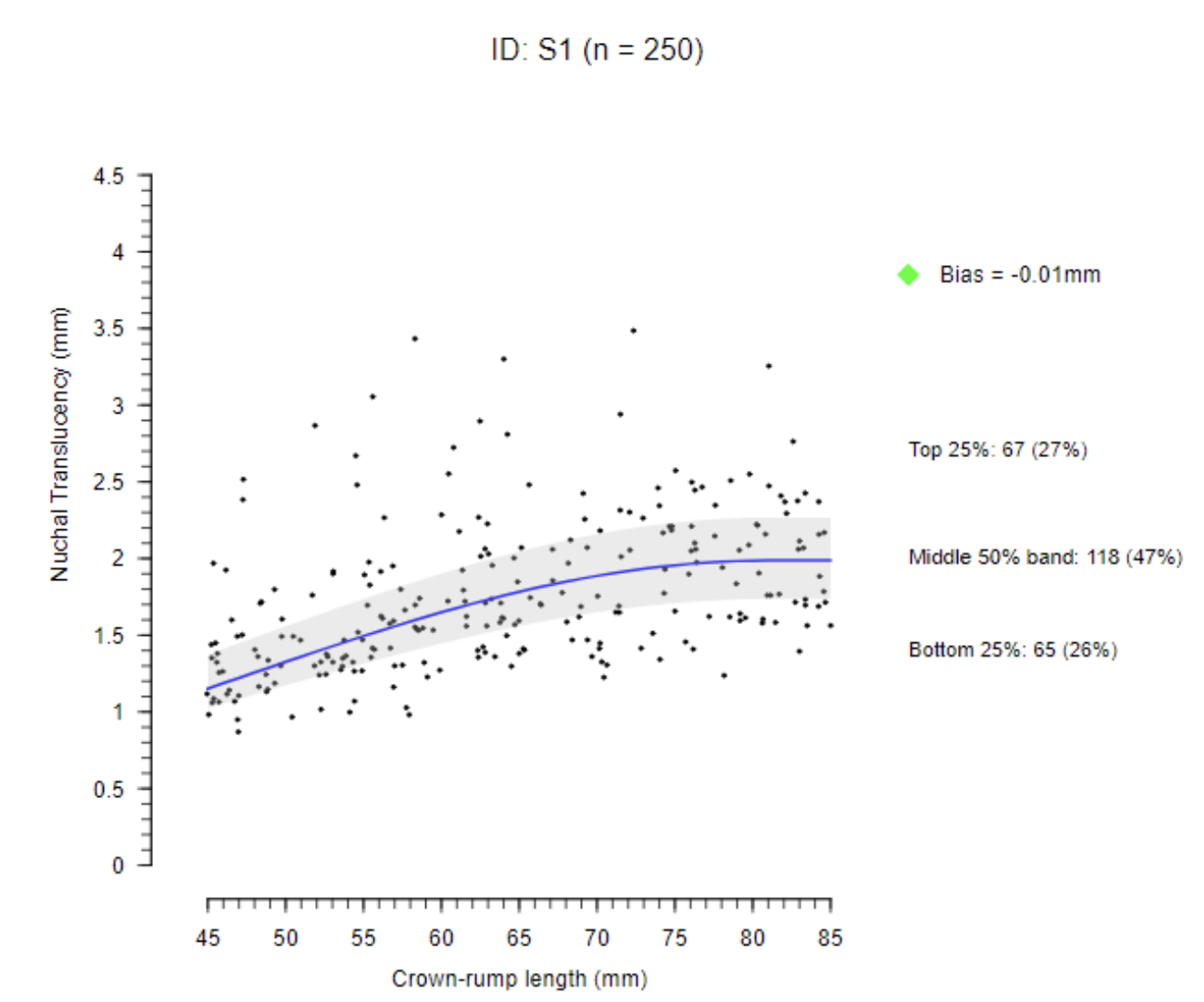
Figure 1: A feedback plot with a green flag for normal bias and spread. Courtesy of NHS FASP (2022).
We all know that as healthcare professionals we should welcome peer review as part of quality assurance and improvement at all levels of practice. Despite this many of us struggle to view peer review in a positive light. We worry about receiving constructive feedback. I would however argue that as modern professionals we need to develop professional resilience and recognise there will always be ways that we can improve, so learn to embrace constructive critical peer review.
Difficult
An example of this is receiving a red flag for negative/positive bias from DQASS, this can be difficult to deal with especially when unforeseen. I would encourage sonographers who find themselves in this position to use it as an opportunity to pause and reflect. Although we need to the recognise the importance of correcting bias going forward to optimise detection rates, and avoid false negative or false positive screening results, it is important that the sonographer effected does not panic about their red flag. With the help of the SSS the sonographer has 12 weeks to complete an action plan and submit a further 25 paired measurements to DQASS.
Recommendations
I would recommend:
- Using your SSS to understand your bias.
- Revisiting the basics by repeating the e-learning module.
- Reviewing images with your SSS, even if your images are acceptable, are there ways that they can be improved? Could you magnify the image slightly more? Could you be more aware of not to include the zygoma in your images?
- Experiment with your machine presets, as these can impact on the results. Try reducing the dynamic range, using focal magnification for calliper placement and/or switching off compound imaging to see if it improves your images?
These modifications might be small, but a 0.1mm change in measurement may be enough to improve bias.
Above all, if sonographers feel able to, we should be open with our colleagues – talk about your experience of critical feedback. We will all receive critical feedback at some point during our careers. There is no such thing as the perfect sonographer. The key is how we use that feedback to better ourselves, keep learning and improving.
Related News
 People
PeopleCrossing borders
Gill Harrison, the SoR's professional officer for ultrasound, reports from the first ultra...
 Ultrasound
UltrasoundAccess to maternity ultrasound appointments for accompanying partners
SoR members are reporting rumours of a new deadline for enabling support person attendance...
 Ultrasound
UltrasoundOvert and covert recording of sonographers performing NHS obstetric ultrasound examinations
Society issues guidance to support local policy development
 Ultrasound
UltrasoundSonographers and patients co-produce obstetric scan ‘etiquette’ statement
‘Covid-19 has given us the chance to re-set our relationship’